


Why have there been so few COVID deaths in Japan?


One of the biggest puzzles of the pandemic is why there have been so few COVID deaths in East Asia, and more specifically in Japan. According to the official death numbers given by Our World in Data, all five advanced East Asian economies – Japan, South Korea, Singapore, Hong Kong and Taiwan – have had fewer than 150 COVID deaths per million people, which is lower than every country in Europe except Iceland. (And the four “Asian Tigers” have had lower death rates than Iceland.)
We can also look at excess deaths – the difference between the number of deaths we observed during the pandemic, and the number we would have expected based on a recent average or trend. According to estimates published by Ariel Karlinsky and Dmitry Kobak on 30th June, excess deaths in the advanced East Asian economies range from –4% in Taiwan to 4% in Hong Kong. By contrast, the range in Europe is –4% in Norway to 43% in North Macedonia, with most countries falling in the interval 10–30%. Here’s the relevant chart:
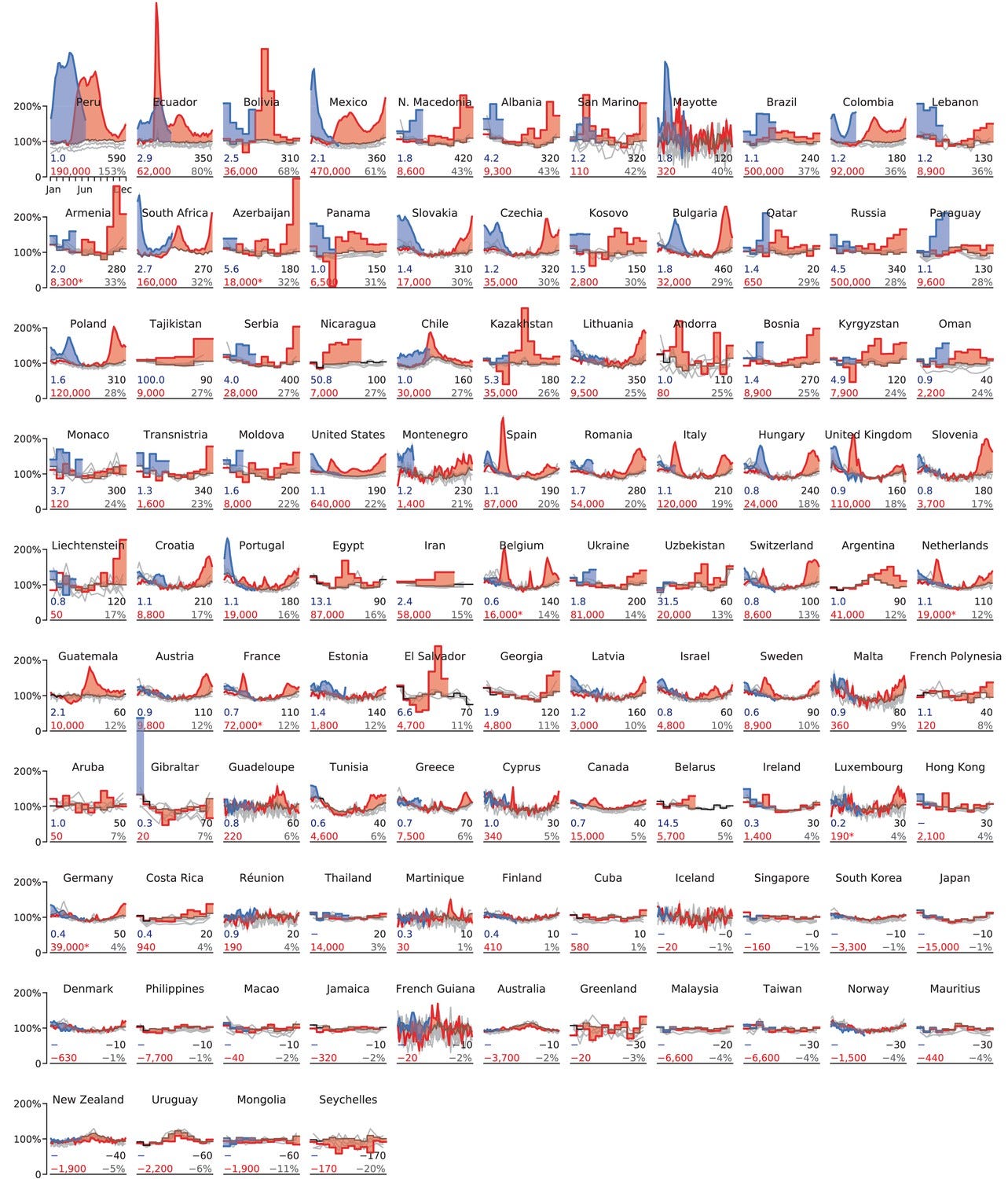
Karlinsky and Kobak’s figures indicate that all the countries in South East Asia have also seen relatively few excess deaths. However, this may be changing with the arrival of the Delta variant. For example, in the latest updates, there were noticeable upticks in both Thailand and the Philippines. The latest figures for Japan show a very slight increase, but that’s up from negative excess mortality last year.
Japan’s low death rate is particularly surprising. While the “Asian Tigers” used a combination of strict border controls, rigorous contacting tracing and selective economic restrictions to achieve containment, Japan took practically no measures – aside from border screening – until quite recently. (And Japan’s border screening is hardly relevant, since the country has had sustained community transmission.) Compared to Europe, where most countries were under lockdown for months, Japan did almost nothing.
According to the Oxford Blavatnik School’s COVID-19 Government Response Tracker, Japan has the 27th lowest average stringency index in the world. Only one economically advanced country that did not achieve containment has a lower score (Liechtenstein). For example, although Taiwan’s score is slightly lower, that country had almost zero cases until the outbreak in May of this year, meaning there was less need for restrictions. Most of the 26 countries below Japan are developing economies that could not afford to lockdown.
Compare Japan and the UK. Since the start of the pandemic, the UK has had 180 days of mandatory stay-at-home orders, and 506 days of mandatory business closures (in at least part of the country). By contrast, Japan has had zero days of mandatory stay-at-home orders, and only 112 days of mandatory business closures (all of which were in 2021). So Japan had zero days of mandatory stay-at-home orders and zero days of mandatory business closures last year. Yet the two countries’ official death curves look like this:

Why have there been so few COVID deaths in Japan? One explanation that’s popular on social media is lack of obesity. According to the CIA World Factbook, Japan’s obesity rate is only 4.3%, the 7th lowest. (The UK’s, by contrast, is 27.8%.) However, as I explained in a recent article, I don’t find this explanation convincing. Although obesity does increase one’s risk of death from COVID, the effect is relatively modest, at least compared to that of age.
For example, in this study based on data from England, obese people were overrepresented among those who died of COVID by a factor of 1.2. Yet people aged over 80 were overrepresented by a factor of 9.2. What’s more, 71% of those who died were not obese, and 39% were not even overweight. Although Japan doesn’t have many overweight people, it does have a lot of people aged over 80 (the highest fraction of any country, in fact). So lack of obesity can’t explain more than a small part of the difference between Japan’s death rate and the UK’s.
One proximate reason why Japan has had so few COVID deaths is that so few people there have been infected. Although this is apparent from looking at official data on cases, it was always possible that Japan simply didn’t test enough. One unpublished study gave a seroprevalence of 47% among a sample of Tokyo office workers in late June of 2020. However, other studies have reported much lower figures, which are in line with the official data on cases. For example, a study of Tokyo healthcare workers in July of 2020 found that just 0.16% were seropositive. Another study by the same researchers yielded an estimate of 0.7% for October–December of 2020.
Japan’s official case curve is shown below. There have been five “waves” in total, of which the most recent is by far the biggest. The first three retreated without any real lockdown measures (aside from temporary school closures) being imposed. And the last two waves have retreated in the absence of any mandatory stay-at-home orders. This, of course, is despite the greater transmissibility of the Delta variant, and the ostensibly low number of people already immune.

Why then have so few Japanese people been infected? One possibility is they simply changed their behaviour voluntarily, thereby curtailing viral transmission. While this is almost certainly true to an extent, it’s unlikely to be the whole story. Given that Japan had almost no lockdown measures in place until recently, voluntary behaviour changes would have to be very large to explain the absence of a major epidemic. Indeed, most European countries saw considerably higher levels of transmission when they were under full lockdown. And note that unlike Norway and Finland (which did impose lockdowns in 2020), Japan is a large, dense, highly connected economy.
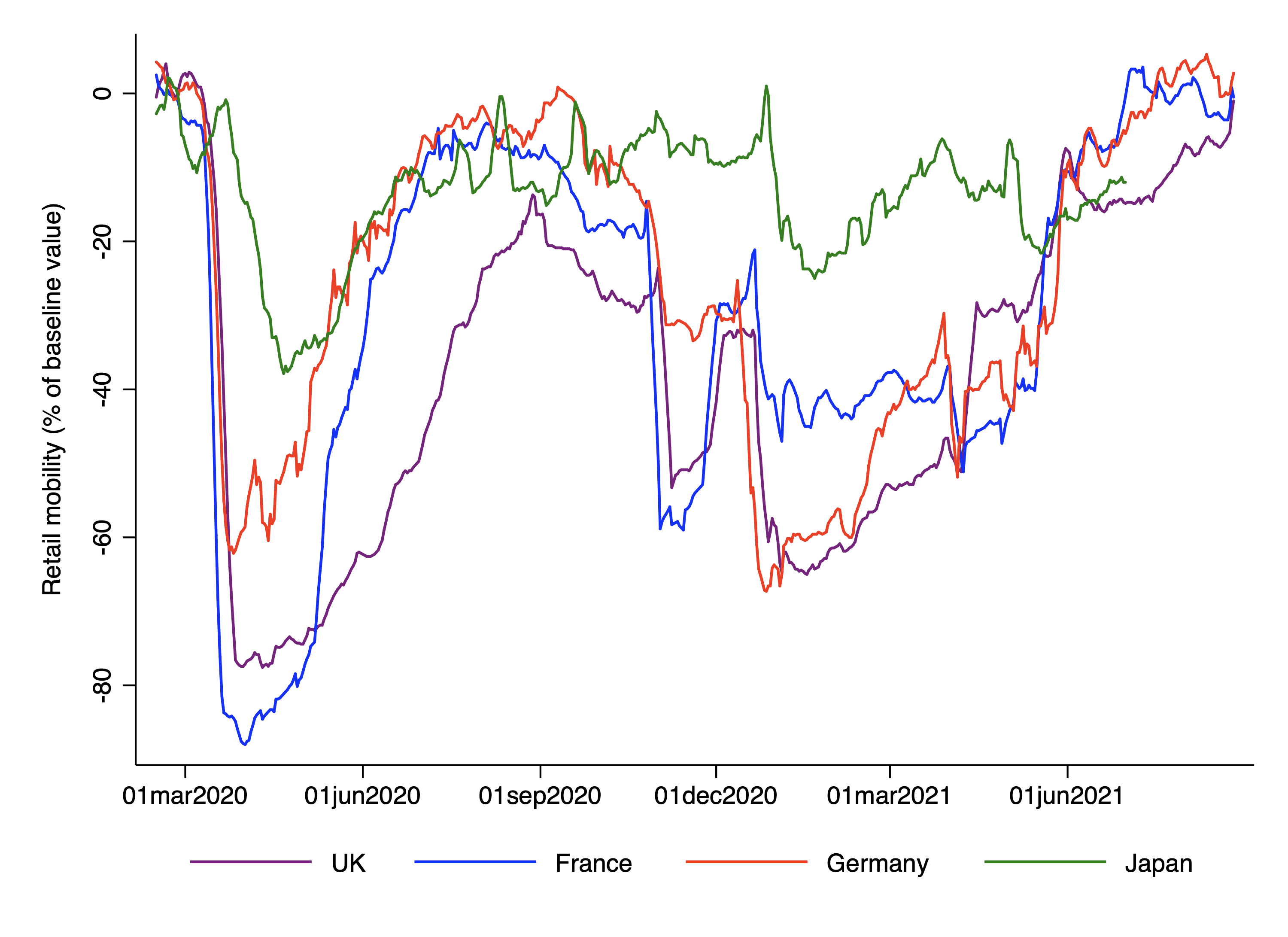
We can get some insight into voluntary behaviour changes using the Google mobility index, which quantifies people’s movements based on smartphone data. The chart below compares retail and recreation mobility in three large European countries and Japan. Somewhat contrary to expectation, Japan saw the least change in mobility up until the summer of 2021. While the lines are closer together on the plots for workplace and residential mobility, there’s no evidence that Japanese people changed their mobility more than the French, Brits or Germans.
Of course, the Google mobility index doesn’t capture all aspects of behaviour. It’s plausible that, although Japanese people didn’t move around substantially less, they did change their behaviour in other ways. Throughout the pandemic, the Japanese government has been telling people to avoid the “three Cs”: closed spaces with poor ventilation; crowded places with many people; and close-contact settings like conversations. If Japanese people were more likely to follow these rather sensible rules, they could have reduced viral transmission to a greater extent than the Google mobility data would suggest. However, I’m not convinced that such subtle shifts in behaviour can explain the absence of a major epidemic.
Another possibility is that Japanese people (and perhaps East Asians in general) have greater prior immunity to COVID-19, which makes them less likely to become infected and/or less likely to transmit the virus. Back in June of last year, Japan’s Deputy Prime Minister Taro Aso caused a minor controversy when he attributed the country’s low death rate to “mindo”, which has been variously translated as “cultural level” or “people’s quality”. (According to the BBC, “It is a concept dating back to Japan's imperial era and denotes a sense of racial superiority”.)
However, even the BBC had to admit there might be “something about Japan that is different”. They quote a Tokyo University professor, who concluded – after studying how his patients react to SARS-CoV-2 – that they may have been exposed to a similar virus before. (The article quotes another academic who is sceptical of this explanation.) In a separate piece, the Wall Street Journal quotes the highest-ranking doctor in the Japanese Ministry of Health, Labor and Welfare as saying that East Asians might have greater prior immunity COVID-19. He cautioned, however, that “there aren’t any solid studies to back up the idea”. The Economist has also entertained the theory that East Asians benefit from prior immunity.
We already know that some individuals have “cross-reactive immunity” to SARS-CoV-2, and that having recently been infected by another common cold coronavirus (CCC) is associated with less severe COVID-19. A recent study published in Science found that cross-reactive immunity declines with age, which “may contribute to the increased susceptibility of elderly to severe COVID-19”. And an earlier study noted that “pre-existing T cell immunity is related to CCC exposure”, leading to the “speculative hypothesis that differences in CCC geo-distribution might correlate with burden of COVID-19 disease severity”.
Reasonable speculation is all well and good. But is there any actual evidence that East Asians in general or Japanese people in particular have greater prior immunity to SARS-CoV-2? The only study I’m aware of is one in Current Biology titled ‘An ancient viral epidemic involving host coronavirus interacting genes more than 20,000 years ago in East Asia’. The authors found evidence of selection for genes encoding proteins that interact with human coronaviruses, but only in East Asian populations. However, they claim their results do “not necessarily imply any difference in genetic susceptibility between different human populations”. So it’s hardly a smoking gun.
What’s more, differences in prior immunity across populations need not be genetic in origin. They could be due to differences in exposure to other viruses during the course of individuals’ lives. Perhaps a closely related virus spread through East Asia at some point during the last couple of decades. Or perhaps such viruses frequently circulate in East Asia, only sometimes reaching other parts of the world. One way of testing this hypothesis would be to compare East Asians living in East Asia with those living in Western countries.
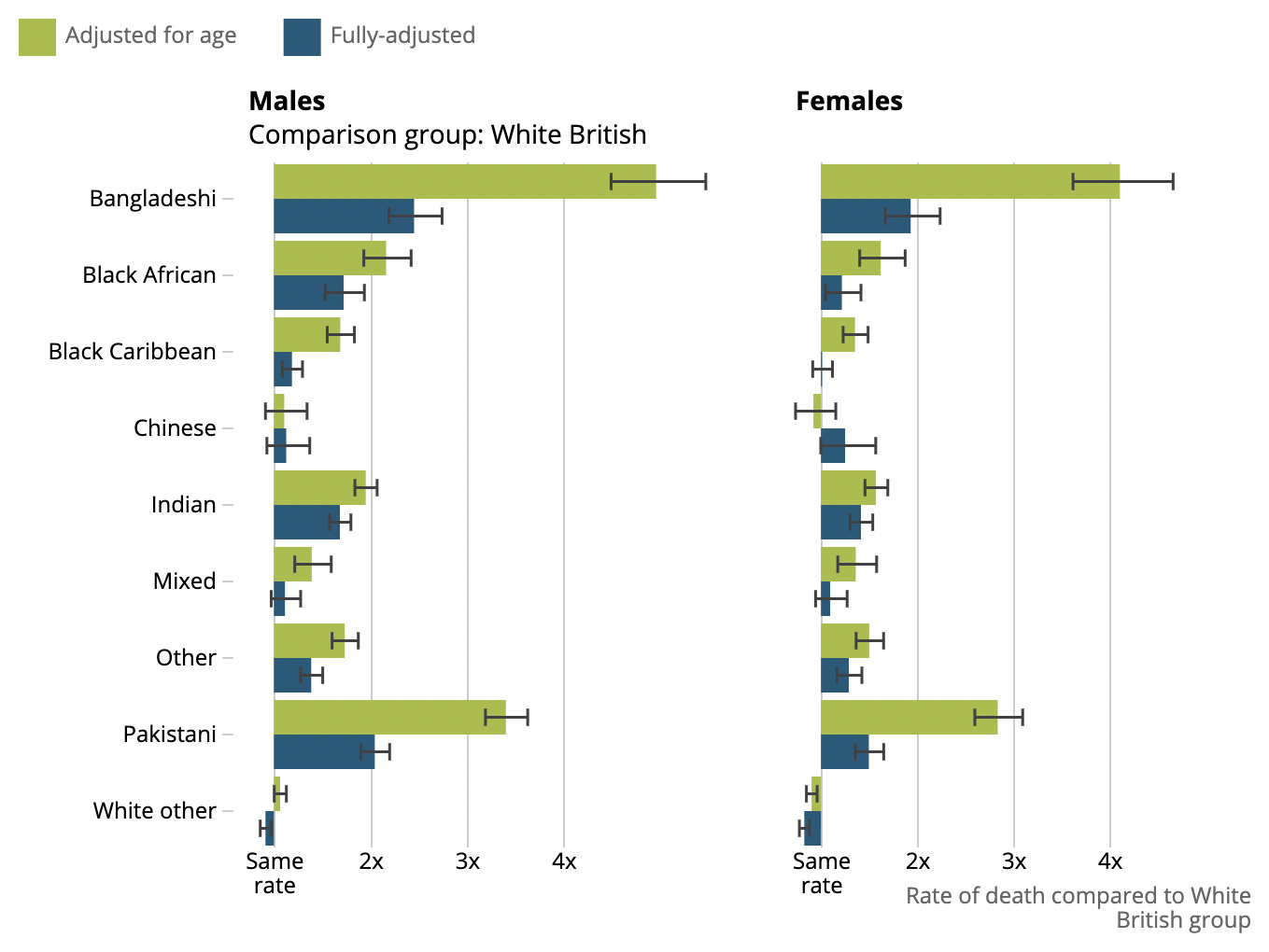
As a matter of fact, this has been done in Britain and the United States, and the results suggest there aren’t genetic differences in susceptibility between Europeans and East Asians. According to the CDC, the age-adjusted COVID death rate for Asian Americans is equal to that for white Americans. Similarly, the UK’s Office for National Statistics has found that the COVID death rate for Chinese Britons is approximately the same as that for White Britons, after adjusting for basic demographic characteristics (see chart below). Unfortunately, there aren’t enough Japanese people in Britain to get a decent sized sample.
Of course, these findings could be reconciled with genetic differences in prior immunity if such immunity only concerned one’s propensity to become infected and/or to transmit the virus. In other words, East Asians could be less likely to catch and transmit the virus, but just as likely to become severely ill conditional on catching it. This scenario is not entirely implausible. East Asians comprise a small share of both the British and American populations, which means the level of transmission is mostly determined by the characteristics of the 95% of people who aren’t East Asian. Once again, however, direct evidence for the hypothesis is lacking.
Japan has one of the lowest COVID death rates in the world, despite being a large, dense, highly connected economy; and despite imposing almost no lockdown measures until quite recently. The country has had sustained community transmission, but each epidemic wave retreated before a large number of people became severely ill. It’s possible that Japan’s death rate will increase sharply in the coming months, although this seems unlikely now that almost 50% of the population is fully vaccinated.
We don’t yet have a good explanation for why Japan has had so few COVID deaths. Lack of obesity can only explain a small part of the difference, and in any case you might expect this would be compensated by Japan’s sizeable elderly population. While voluntary behaviour change – including adherence to the “three Cs” – almost certainly plays a role, I’m not convinced this alone can explain the absence of a major epidemic. Rather, I suspect greater prior immunity is also a factor. However, both of these hypotheses remain speculative for the time being.
Image: Morio, View of Shinjuku skyscrapers and Mount Fuji, 2009
The New Puritans
Anne Applebaum has written an excellent essay on cancel culture in The Atlantic. I don’t agree with every word (she’s slightly more charitable to Critical Race Theory than I would be) but it’s well worth reading. Here’s an excerpt:
The censoriousness, the shunning, the ritualized apologies, the public sacrifices—these are rather typical behaviors in illiberal societies with rigid cultural codes, enforced by heavy peer pressure. This is a story of moral panic, of cultural institutions policing or purifying themselves in the face of disapproving crowds. The crowds are no longer literal, as they once were in Salem, but rather online mobs, organized via Twitter, Facebook, or sometimes internal company Slack channels.
The Daily Sceptic
I’ve written five more posts since last time. The first asks whether lack of obesity can explain low COVID-19 death rates in East Asia. The second summarises a philosophy paper arguing that justifications for lockdown have implications most people would not accept. The third argues that the Bangladesh mask study is a massive missed opportunity. The fourth argues that it’s unethical to vaccinate 12–15 year olds when such a small share of the population in poor countries has been offered a vaccine. The fifth notes that recent coverage of the lab leak theory has been driven by right-wing media.
Thanks for reading. If you found this newsletter useful, please share it with your friends. And please consider subscribing if you haven’t done so already.