


How to fix low back pain
...using this one simple trick. Chiropractors hate him!


NOTE: I now write for Aporia Magazine. Please sign up there!
It’s cold out. You’re carrying a full garbage bag to the bin outside. As you trudge along the gravel path, a single plastic wrapper falls out of the bag and gently flutters to the ground. You place the bag down, and bend over to pick it up. But then disaster strikes! You feel a sudden shooting pain, and the sensation of something popping in your lower back. Your muscles begin to seize up. What is usually the most trivial of tasks – retrieving a small object from the floor – now seems like a herculean undertaking. You look at the wrapper in dismay, and whisper “You’ve won this round”, before hobbling back inside.
Many of us have had an experience like this at least once in our lives. As a regular gym-goer, I can tell you that it’s happened to me several times, and I’m only in my 30s. The intense pain, and the feeling that someone’s glued your vertebrae together to prevent any movement, typically lasts a few days. (During this time, you find it necessary to walk around like an overly upright penguin.) As the pain and tightness gradually subside, you rediscover that humans can flex their spines; life – you realise – doesn’t have to be lived in a perfectly vertical position. After a couple of weeks, you’re back to full health. And the plastic wrapper is in the bin, where it belongs.
Why am I talking about low back pain? It’s not the worst thing in the world, you might say. Well, actually it is the worst thing in the world, as this remarkable map shows:
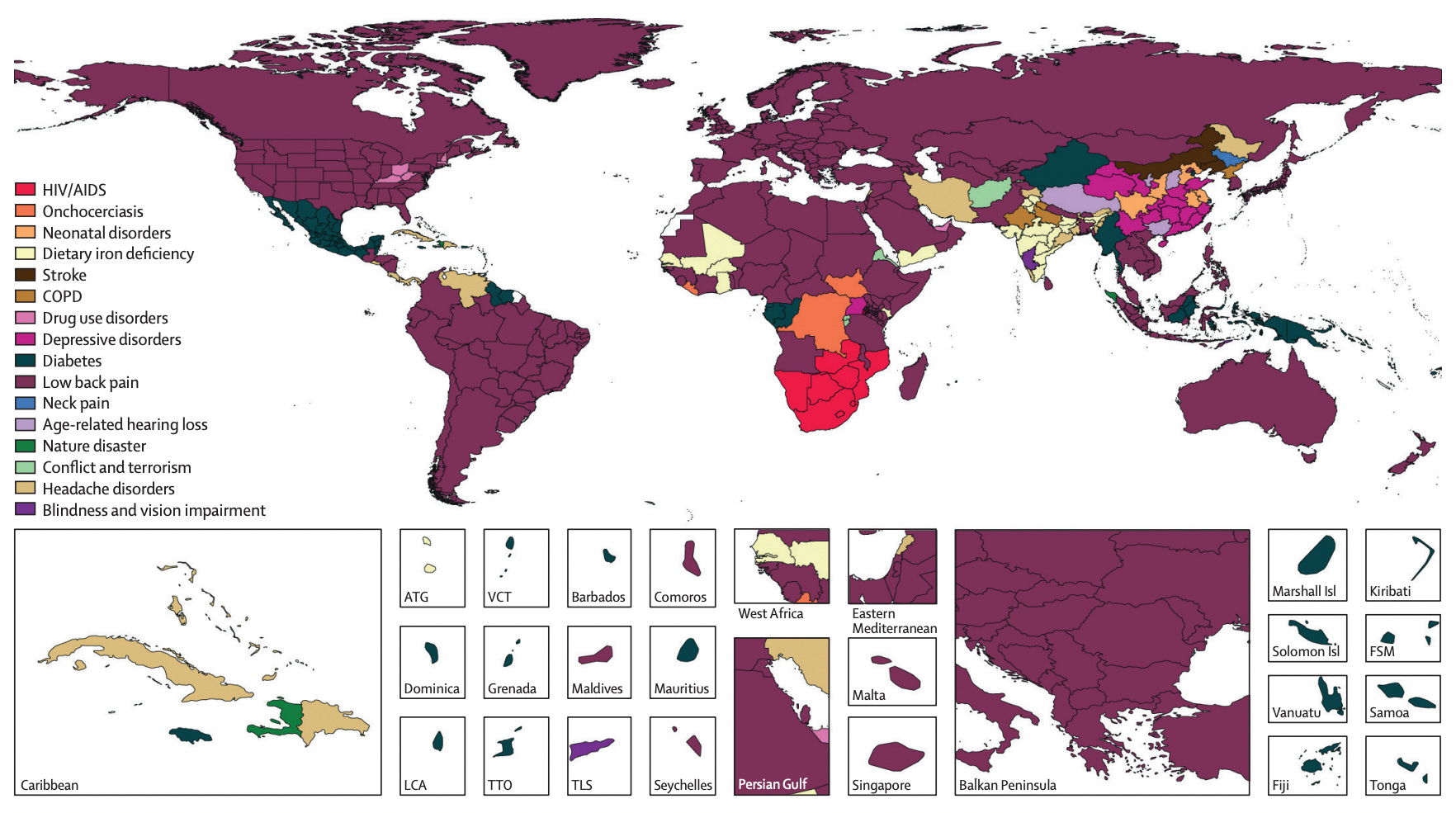
The map is taken from a 2018 paper in The Lancet. It simply shows, for each country in the world, which of the conditions on the left-hand side is the biggest contributor to years lived with a disability. (I’ll explain exactly how that’s calculated in a second.) Almost the entire map is shaded purple, indicating that low back pain is the biggest contributor to years lived with a disability in the vast majority of countries. As I said, low back pain is the worst thing in the world… that doesn’t kill you.
Interestingly, most of Latin America and much of Africa is shaded purple, meaning that – even in the developing world – low back pain is a major issue. There are three world regions where conditions other than low back pain are bigger contributors to years lived with a disability. In Southern Africa, HIV/AIDS is more significant; in India, iron deficiency is more significant; and in China, depressive disorders are more significant. But in practically all of North America, South America, Europe, North Africa, Central Asia and South East Asia, low back pain is the number one issue.
According to an earlier 2012 paper, which reviewed 165 studies from 54 countries, at least 40% of people experience low back pain at least once in their lives (and the figure might be as high as 70% for industrialised countries). Interestingly, it’s slightly more common among women than among men.
So what exactly is ‘years lived with a disability’? It’s an important measure, which is one of two inputs into the well-known DALY statistic (disability-adjusted life years). When it comes to a particular condition, you calculate years lived with a disability by multiplying the prevalence of that condition by the corresponding disability weight. Prevalence is straightforward: how many people time are suffering from the condition at a certain point in time? Disability weights are slightly more complicated.
They basically quantify how debilitating different conditions are, which allows us to compare them more meaningfully. If we didn’t use disability weights, we’d just be comparing the prevalence of different conditions, and we’d have to say that one year lived with total blindness is the same as one year lived with mild low back pain. This is implausible to say the least; living with total blindness is a lot more debilitating.
There are different ways of obtaining disability weights. For example, you could just ask medical professionals to assign them, based on their knowledge of different conditions. However, the methodology used for the Global Burden of Disease Study (from which the above map comes) is slightly more complicated, and doesn’t hinge on the assumption that specialists have unique insight into which disabilities are worst.
As explained in this 2015 paper, researchers administer a survey to large nationally representative samples from several countries. Respondents are asked to consider two hypothetical individuals, each suffering from a different condition, the main symptoms and functional impacts of which are described. They are asked to say which of the two individuals they regard as healthier. This is repeated ten or twenty times per respondent, with conditions selected randomly from a list of several hundred. Because there are thousands of respondents per sample, the surveys generate enough data to quantify the severity of a large number of conditions, even though each respondent gives only ten or twenty responses. Precise numerical weights are obtained by fitting models to the data, which take account of the relative frequency of answers to each hypothetical comparison.
In the aforementioned study, the estimated weights range from 0.003 for ‘mild distance vision impairment’ to 0.778 for ‘acute schizophrenia’. Note: this implies that 259 years lived with mild distance vision impairment is equivalent to one year lived with acute schizophrenia. There are six categories for low back pain. ‘Mild low back pain’ has a weight of 0.020 (about six times worse than mild distance vision impairment), whereas ‘most severe low back pain with accompanying leg pain’ has a weight of 0.384 (about half as bad as schizophrenia). Full results are available in Table 2.
Another thing to note is that the map is based on age-standardised years lived with disability. In other words, the colour reflects the condition that contributes most to years lived with a disability, assuming that every country has the same age-structure. This matters because some conditions are quite common in middle age, whereas others are only common at advanced ages. The World Standard Population (which I believe is the one they used for standardisation) has a slightly younger age-structure than most developed countries, since it’s designed to be a kind of global average. Given that low back pain is more common among older people, the pattern in the map is therefore unlikely to be an artefact of the standardisation procedure.
So how do you fix low back pain? Well, I got interested in this subject because I recently had an experience not dissimilar from the one described in the opening paragraph. You see, I was in the gym bench-pressing four times my bodyweight and something just gave way. (Note: some details in the preceding sentence may have been embellished.) This wasn’t the first or even the second time I’d tweaked my back lifting weights, so you can imagine my annoyance (mostly at myself).
Once the initial, penguin-walking phase was over, I assumed I’d be back in business. To my great frustration, however, this proved not to be the case. Although the intense pain that is characteristic of acute injury had dissipated, a certain degree of tightness and immobility remained. More than six weeks after the original incident, I still had trouble bending forward to pick things up. Would this be my life from here on out, I wondered. Was I now a nominally youngish man with the functional abilities of a senior citizen?
And I thought I’d done everything right. I’d stayed away from the gym for two full weeks, while remaining reasonably active (in the form of daily walks and other “light activity”). I’d been careful not to aggravate the situation; the body squat had become my modus operandi for retrieving floor-bound objects, and I’d studiously avoided any movements that caused pain in the affected the area. What more did my lower back want?
So I turned to the internet for advice. Not before long, I came upon a video lecture by a gentleman named Austin Baraki, which turned out to be immensely helpful. At this point, I could simply say: go watch the lecture, especially if you’re suffering from low back pain now, or you’re the kind of person who’s liable to get a back injury at some point (e.g., gym user, tree feller, elephant lifter). However, I’ll do my best to summarise the main points here.
Baraki is a medical doctor, who has studied musculoskeletal pain for many years. And unlike many practitioners in this area, he actually has some “skin in the game”, so to speak, in that he’s also a successful powerlifter. (Here’s a video of him squatting 520 pounds, benching 385 pounds and deadlifting 600 pounds.)
In the lecture, he makes a number of salient points. For example, results from various diagnostic tools (e.g., X-rays, CT scans, MRI scans) correlate weakly or not at all with experience of low back pain. Second, most drugs (including painkillers and “muscle relaxants”) have little or no effect on low back pain, and any effect they do have is generally limited to the acute phase of injury. Third, the trajectory of symptoms during the acute phase can’t really be altered; if you tweak your back, you’re going to be in pain for a few days (at least to some extent).
However, the most interesting – and for me most informative – aspect of Baraki’s lecture is what he has to say about the meaning of pain. I don’t mean the philosophical “meaning”, but rather what pain tells you about the health and integrity of structures in your lower back. Hence if you don’t want to sit through the entire lecture, which is just over an hour, I’d recommend watching the five minutes from 45:00 to 50:00.
Baraki notes that, contrary to popular myth, pain does not necessarily mean damage. If you’re recovering from a back injury, and you start to feel pain while bending over, this doesn’t mean you’re re-damaging the affected area, and it doesn’t mean your body “isn’t ready” for that movement. “This idea that we should just avoid things that hurt,” Baraki states, “I’m not a fan of it.” As he explains, pain is more an indication of threat than of actual damage. And he says that pretty much the worst thing you can do when recovering from a back injury is to immobilise the lower back, so that you never experience any pain or discomfort. (Of course, this doesn’t mean you should jump straight back into 500 pound deadlifts.)
I implemented Baraki’s advice over the following two weeks. Rather than avoiding movements that elicited pain or tightness, I actively performed them: slowly at first, and without any resistance (i.e., just using my bodyweight). The first few times, it felt pretty awkward. But after only a couple of days, my back felt noticeably better. I then gradually added of resistance in the form 5, 10 and 15 kilo dumbbells, so I was essentially performing very light dumbbell deadlifts. By the end of the two weeks, the situation had improved dramatically.
If you were to plot my pain levels over time, the line would begin by shooting up on the day of the injury; it would then come down gradually as the acute phase ended; it would remain flat but above zero for the next five weeks; and it would then come down to almost zero over the last two weeks (when I was performing the movements describe above). I wouldn’t say my back has completely recovered, but it’s a lot better than before I implemented Baraki’s advice. As it turns out, the “one simple trick” to fix low back pain, at least in my case, was to get the right information.
Image: Lucas Cranach the Elder, Hercules and Atlas, 1537
The Daily Sceptic
I’ve written five more posts since last time. The first puts the UK’s pandemic death toll into perspective. The second argues that a recent viral tweet opposing “herd immunity” gets pretty much everything wrong. The third asks whether we are starting to see the impact of lockdown on mortality. The fourth notes that some people are still pushing ‘Zero Covid’. The fifth summarises a recent study finding that experts are worse than non-experts at predicting case and death numbers.
Thanks for reading. If you found this newsletter useful, please share it with your friends. And please consider subscribing if you haven’t done so already.